Items
topic_interest is exactly
2AZs
-
 2021-04-20
2021-04-20JOTPY Exhibit: "Arizona's COVID-19 Pandemics" by James Rayroux
While working as a curatorial intern on ASU's 'A Journal of the Plague Year' COVID-19 archive, I created this exhibit on the pandemic experience within the state. In addition to obvious, overarching realities such as socioeconomic status and immediate access to healthcare systems, I initially believed one of the greatest deciding factors that determined one's experience in Arizona was an individual's residence in either predominantly urban or rural environments. The proposed exhibit had been originally titled "A Tale of Two Arizonas" to pay respect to Charles Dickens and the differing realities experienced here. To test my proposed hypothesis, I went about finding data, stories, and submissions that substantiated or disputed my premise. Within a short time, I had identified four distinct environmental drivers of personal pandemic experiences; to me, that indicated the existence of many more I hadn't yet found or had overlooked along the way. My evidence suggested a minimum of four pandemic locales: Urban, Rural, Border, and Tribal within the State of Arizona and its fifteen counties. The recorded health data and personal experiences demonstrated the naivete of my initial hypothesis, and I retitled the exhibit: "Arizona's COVID-19 Pandemics." The Exhibit Background section illustrates the vast dichotomies within Arizona in terms of population density and access to healthcare facilities. Given the virus's respiratory nature, these factors seemed especially relevant to driving diverse local experiences. I chose to include a flyer from the Coconino County Health and Human Services' "Face It! Masks Save Lives" campaign. The flyer included a specific line to "Stay Home When Sick" that seemed to illustrate a different public health paradigm than the broader "stay home" orders from Maricopa and Pima county. This section also features an image of Sedona's red rocks and a portion of The Wave to remind visitors of the wide-open rural areas accessible to all, as well as those with cultural significance to the Native American tribes and limited access to the general public. The next section asks a short, five-question survey in which visitors may participate. The Silver Linings piece features a short audio clip of a father and husband discussing some unexpected benefits of the pandemic. Visitors may explore additional Silver Linings stories and submit their own experience. The Tséhootsooí Medical Center piece seeks to illustrate the different pandemic experience on the state's tribal lands. I hoped to inspire some relevant emotional turmoil for the visitors through the piece's visual presentation. I wanted to create a series of waves with quotes from the medical center's healthcare workers. I hoped visitors' attention would be drawn to the large, bolded key words, and that they would first experience the segments out of sequence because of that. After potentially feeling a sense of chaos, they might settle themselves into a deliberate reading of the texts and find their own order within the experiences provided here. This piece allows further exploration of Native submissions and topics, a review of an additional related news article, and a submission prompt that invites visitors to offer guidance to hospital managers. The next piece illustrates the differences between mask mandates in communities across Arizona. In addition to hearing an audio clip of interviews with mayors and a public health official, visitors can explore additional submissions related to mask mandates and submit their thoughts on statewide mandates. The Arizona Department of Health Services provides zip-code specific infection data on its website, and the wide array of known case infections therein further illustrates potential dichotomies across the state. In working to include and represent this data in a consumable way, I encountered inconsistencies with tribal data. The nation's Indian tribes are overseen by Indian Health Services, a federal public health agency, and it does not collect or report data in the same manner as the State of Arizona or its counties. At first glance, the data would seem to suggest that tribal areas had less severe pandemic experiences than the rural and urban areas, which was not objectively true. I wanted to offer the unedited data to visitors, allow them to drawn their own conclusions, and invite them to offer their thoughts on what potential misunderstandings might emanate from these reporting differences. Visitors may also choose to review the foundational data from this piece, as well. I used the following two sections to offer submission prompts about the visitor's overall pandemic experience as a function of their location, as well as what they might have done if placed in charge of their city, county, or state during this pandemic. A diverse Search section allows visitors to explore additional topics of interest to them. 23 hyperlinks offer pre-defined search parameters. An Advanced Search link allows self-defined research, and a Join The Staff link connects visitors with opportunities to work within the JOTPY archive. A final section asks visitors to provide feedback on the exhibit, its content, and the pandemic in general. Both surveys within the exhibit will display overall results to visitors who participate in them. Through this process, I found incredible amounts and diversity of data outside the archive that spoke to these generally localized experiences, but not that much yet within the archive explained what Arizonans had experienced outside the state's urban environments. I created a call for submissions and delivered it to fifty rural entities that might help support the effort to collect and preserve more rural Arizona stories. Between all the local libraries, historical societies, museums, small-town mayors, and county health officials to whom I asked for help, I am optimistic the archive will better represent all Arizonans in the coming months and years. Despite the exhibit having been created, I ensured its internal search features would include future submissions and allow the exhibit to remain relevant long after its release. -
 2021-04-20
2021-04-20Northern Arizona's Coconino County "Face It" Mask Campaign and Online Toolbox
The Coconino County Health & Human Services department created its "Face It" campaign in 2020 to promote the use of masks and face coverings in their communities. The following webpage is for the campaign's digital "toolbox" to give the public access to official signage for display to customers, the public, and employees to address mask use issues. -
 2021-04-15
2021-04-15News Article: The Mother Road welcomes Route 66 Bike Week: Event aims to boost small businesses
By Travis Rains, Kingman Daily Miner, 15 April 2021 Communities and businesses along and near the Mother Road wanted in on the action that is Route 66 Bike Week – five days of activities, games, discounts, scenic biking and more set for April 21-25 along the historic highway from Needles, California to Seligman. Event organizer Rob Borden is no stranger to motorcycle rallies as the owner of Saddle Sore Ranch, located between mile markers 36 and 37 on Route 66, approximately 17 miles from Kingman. But this is the first year for Route 66 Bike Week, which has seen the expansion of what has been dubbed the “Laughlin Loop.” “It kind of started by accident,” Borden said, noting the loop includes Route 66, going through Oatman and down over highways 95 and 68. “It’s just a nice, scenic ride for motorcycle enthusiasts. With the Laughlin River Run not happening, at least not in the past two years, I got a call from Needles, California from their tourism center asking if they could be included in this Laughlin Loop and I said ‘absolutely.’” Borden then received a call from the chamber of commerce in Oatman seeking to be included in the event. Then the City of Kingman and its visitor’s center wanted on board, followed by Seligman. “So then I’m looking at it and I’m like ‘wow, Needles to Seligman,’” Borden said. “I said ‘why don’t I just do a Route 66 Bike Week,’ and that’s how it happened. That way we can promote all these small businesses down Route 66 that even in normal times they struggle. Now with COVID, of course, they’ve been struggling even more.” So Borden began reaching out to businesses along Route 66 to see if they would be interested in participating by way of deals and discounts for event participants. “They loved the idea and wanted to be a part of it,” he said. “Basically, the idea is rather than just have a stationary event that’s confined to some big parking lot, let’s kind of highlight these businesses up and down Route 66 and get them involved. They’ve put together special offers and discounts, maybe extra effort for bands for bars. Those are different stops on the rally.” Registration for bike week can be completed by going to http://route66bikeweek.com/, with prices ranging from $45 to $48 depending on the package chosen. Borden said there is associated costs for the event that include T-shirts, bike week wristbands and dissemination of the Route 66 Passport, the latter two providing participants with access to discounts from businesses and drawings for prizes, respectively. “So when you show up with your bike week wristband, you’ll get freebies and discounts,” Borden explained. “We’ve got about 20 free drawing stops.” A scavenger hunt is planned as well utilizing the Route 66 Passport. Borden said there will be five different stops along Route 66 at which participants can have their passports stamped. Upon getting all the stamps and presenting them at Rally Central, which is Saddle Sore Ranch, they will receive a free ticket for yet another drawing. Borden also said those wishing to cruise Route 66 during bike week don’t have to register, but that they will not receive access to discounts and more. “The intent there is obviously to bring exposure to Route 66 and all these businesses, and make a big financial impact right here to the area as opposed to some of the big corporate vendors that would come into big motorcycle events,” Borden said. “When they leave, they take the money with them.” Saddle Sore Ranch will play host to biker games and activities throughout Route 66 Bike Week. Those will include poker runs, live music and popular biker contests like a big belly contest. Biker games such as slow races, barrel races, lean-your-bike and more are scheduled as well, as is a blue collar build-off judging and awards ceremony sponsored in part by Cycle Source Magazine. The build-off is a low-budget motorcycle building competition where teams from all over the country had $1,500 and 30 days to build a bike. After the sun goes down, live music will continue, vendors will open up shop and a campfire party will commence. “It’s a lot different than what people are used to with previous motorcycle rallies in the area,” Borden said of Saddle Sore Ranch. “Our venue is more reminiscent of a ‘60s or ‘70s style, easy rider rodeo kind of venue. It’s more of a traditional, old-school biker venue as opposed to the neon lights and things like that of Laughlin. It’s a completely different kind of feel and a breath of fresh air for bikers in the area to give them something to do and something different.” Route 66 Bike Week starts at 10 a.m. Wednesday, April 21 and runs until 10 p.m. Sunday, April 25. For more information on Route 66 Bike Week, go to http://route66bikeweek.com/. -
 2021-04-19
2021-04-19News Article: Navajo Nation reports no COVID-19 deaths for 8th day
By Associated Press, 19 April 2021 WINDOW ROCK (AP) — The Navajo Nation is finding no new COVID-19 related deaths for an eighth consecutive day. The tribe on Sunday afternoon reported seven new virus cases but no additional deaths on the vast reservation. The latest numbers bring the Navajo Nation's pandemic case total to 30,366 with the death toll remaining at 1,262. Tribal officials said 16,477 people have recovered from COVID-19 thus far. The tribe had been easing into reopening but that slowed somewhat after coronavirus variants were confirmed on the reservation, which stretches into New Mexico, Utah and Arizona. Tribal officials urged residents to stay vigilant. Navajo President Jonathan Nez said the tribe recently had a cluster of COVID-19 cases as a result of a family gathering where people were not wearing masks. Tribal public health orders mandate that masks be worn on the reservation and a daily curfew is in effect. Restaurants cannot have dine-in services. Navajo Nation roads also are closed to visitors and tourists, which doesn’t affect travel on state highways that run through the reservation. Meanwhile, health care facilities across the reservation continue to offer the vaccine by appointment or at drive-thru events. -
 2021-04-07
2021-04-07Indian Health Services COVID-19 Infections by Service Area through 04/07/2021
Indian Health Services is an agency of the United States federal government that oversees and administers healthcare to that nation's Native American populations and tribal reservations. This webpage from the Indian Health Services has three sections that address general Coronavirus (COVID-19) information and links, COVID-19 Vaccine Distribution and Administration by IHS Area, and COVID-19 Cases by IHS Area. it also includes a hyperlink to an interactive map for up-to-date COVID-19 Cases by IHS Area: https://maps.ihs.gov/portal/apps/StoryMapBasic/index.html -
 2021-04-08
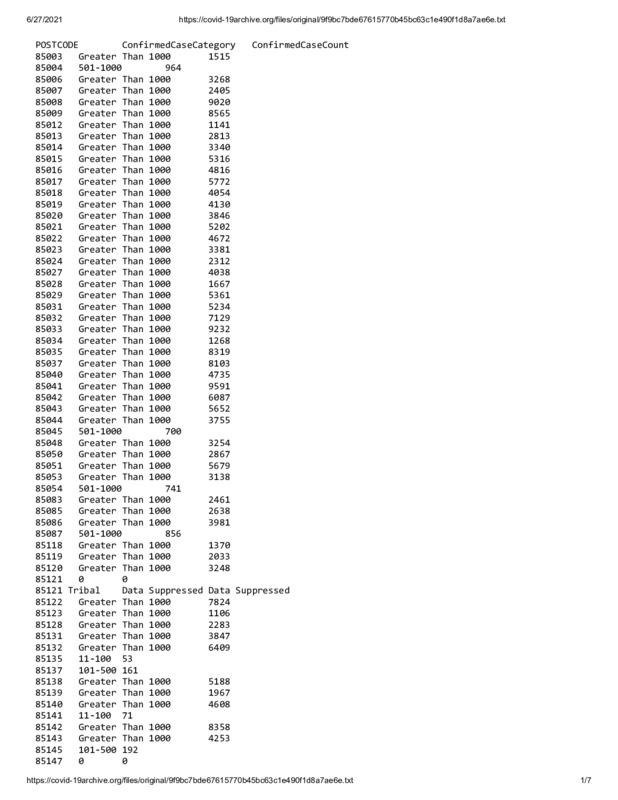
2021-04-08Arizona COVID-19 Infections by Zip Code through 04/08/2021
This text file shows data from the Arizona Department of Health Services for confirmed COVID-19 infections tied to the patient's residential zip code. The data runs through 04/08/2021 and can be searched by "Ctrl + F" and entering specific zip codes. AZDHS suppressed tribal data from this data file prior to its publication on the organization's website. -
 2021-04-04
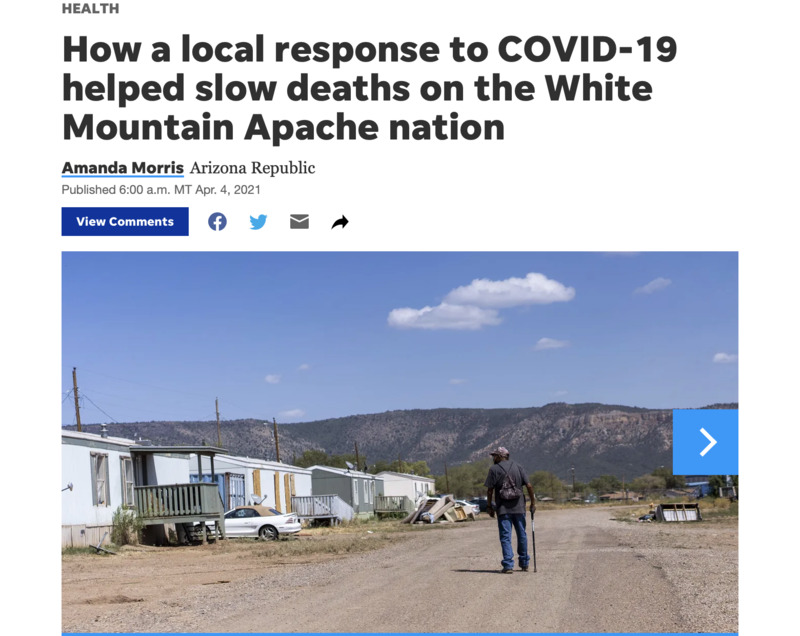
2021-04-04News Article: How a local response to COVID-19 helped slow deaths on the White Mountain Apache nation
By Amanda Morris of the Arizona Republic: When someone on the Fort Apache Indian Reservation receives a confirmed diagnosis of COVID-19, health care workers from the Whiteriver Indian Hospital jump into action. They personally visit the individual's home to test other household members, perform health evaluations on everyone there and trace any other potential contacts at risk for COVID-19 exposure. Health care workers in the community say that could be one reason why, even though the rate of confirmed COVID-19 cases among White Mountain Apache tribal members is nearly triple the state's rate, the death rate is much lower and continues to fall. Over 90% of COVID-19 cases in the White Mountain community are investigated within 24 hours of testing, according to Ryan Close, the director of the Department of Preventative Medicine at the Whiteriver hospital, which is the only hospital on the 1.67 million-acre reservation. "I feel like what we did made a huge difference," Close said. "We evaluated and admitted people aggressively and early. The tribe deserves an incredible amount of credit for mobilizing staff ... to make this response possible, because at some point it would have been very difficult to maintain without their considerable help." The quick response may have also helped the tribe turn the tide against rapid community spread of the virus, which scientists say could have been fueled by a single variant found only in the White Mountain tribal communities. The variant carried a mutation in the spike protein, which scientist theorize could have made it spread more rapidly than other strains of the virus. The number of confirmed COVID-19 cases among White Mountain Apache tribal members accounts for 24% to 28% of their population, according to Close, but the cumulative death rate among known cases is only 1.2%. By comparison, the statewide rate of infection was 11.5% with a 2% death rate among known cases. And over the winter, Close said the rate for the tribe dropped even lower, to about 0.5%. In a community with a high number of individuals with underlying health conditions, the low death rate and work of the tribe has been "remarkable," said David Engelthaler, director of the Translational Genomics Research Institute's infectious disease division in Flagstaff. The death rate also stands out as unusually low when compared with death rates in other Indigenous communities. Indigenous populations have been disproportionally affected by the pandemic. CDC data shows that Indigenous people are 3.5 more likely to be diagnosed with COVID-19 and almost twice as likely to die from COVID-19 than white people. Close credits a proactive strategy to combat COVID-19 that involved rapid contact tracing, in-person health evaluations and frequent outreach to high-risk COVID-19-positive individuals as well as early treatment with monoclonal antibodies and other antiviral therapies. Volunteers and health workers from the White Mountain Apache community were on the Whiteriver hospital's contact tracing team and high-risk COVID-19 outreach team, which Close said helped the team connect better with the people and work faster. One essential part of the team are the tribe's community health representatives, or CHRs, who are members of the community that serve as a cultural bridge between patients and medical establishments. JT Nashio, director of the Community Health Representatives for the tribe, said the "visceral connection" that CHRs have to the community helps them bring cultural awareness to the way questions are asked for contact tracing, which makes the process more effective and allows officials to better distribute information. "On top of that, quite simply, they know how to get around. It’s a big reservation and not all homes are easy to find," Nashio said. "But when you’ve lived here your whole life, you know where to find people. That became invaluable during the tracing and testing push during case surges." Virus mutation may have made it more transmissible When COVID-19 hit the White Mountain Apache nation, it spread rapidly. The community's first documented case was on April 1, 2020, from someone who had likely recently visited the Phoenix area, unknowingly caught COVID-19 and returned, according to Engelthaler. Within the first few weeks, Close said the community experienced a handful of deaths. "We soon had incidence rates that were skyrocketing. Case counts were going up very, very quickly," Close said. It's unclear why the disease spread so rapidly in the community, but the initial strain of COVID-19 that hit the community carried a mutation that Engelthaler believes could have made it more transmissible. "They were seeing the virus just rip through and have an 80 to 90 to 100 percent attack rate," he said. TGen partnered with the tribe and the U.S. Indian Health Services early on to provide tests to diagnose a case of COVID-19 and provide genetic analysis of the virus from each case. It showed one strain of the virus circulating in the tribal community that wasn't present anywhere else in the state. "This virus moved much faster than anything else we were seeing in Arizona at the time," Engelthaler said. "So we actually believe that we had one of these variant strains in Arizona that was causing very large numbers of cases, but it was secluded and maintained really only in that tribal population." The mutation, called the H245Y mutation, occurred in the spike of the virus, which Englethaler said is a "very sensitive" part of the virus where mutations can have a significant impact. Because of the low death rate, Engelthaler said TGen researchers would like to investigate the mutated strain of coronavirus seen among tribal members to see if it is also associated with a lower fatality rate. He acknowledged that other strains of the virus have since entered the community and that the actions of health care workers in the community and at the Whiteriver hospital is also responsible for the lower death rates. 'The earlier you treat an illness, the better' Close's biggest concern was that an outbreak would cause a "tsunami" of sick COVID-19 patients that would run the risk of overwhelming the Whiteriver hospital, which does not have an intensive care unit. Any patients that require intensive care need to be transported to other hospitals in the state. "We're a small hospital, we cannot take a wave of all very acute patients because there aren't enough ventilators in the hospital," Close said. "There aren't enough helicopters in the state to transport people out from our facility to a higher level of care." Within the first few weeks, Close said the community experienced a handful of deaths, and patients who had the poorest outcomes were the ones who self-presented at the hospital — often meaning they waited until they felt sick enough to go to the hospital. "People don't always bring themselves in early enough," Close said. "The earlier you treat an illness, the better." In response to this phenomenon, the hospital started a high-risk outreach program the third week of April. Health care workers regularly visited the homes of anyone who tested positive for COVID-19 and was at high risk for a poor outcome. Close recalls multiple days when he evaluated patients and found their oxygen levels dangerously low, even though they felt fine. It's a condition associated with COVID-19 known as "silent hypoxia," or "happy hypoxia." "They had no sense that they were even ill. They went on to get pretty sick in the hospital, but they survived and you can't help but think to yourself, 'Yeah, that's a life saved,'" Close said. "That person, if they had stayed home another day or another two days would not have done as well. They would have ended up on a ventilator or something." The Arizona Republic previously reported that the effects of the high-risk outreach program and contact tracing led to a fatality rate among tribal members of 1.6% last June, which was less than the state's rate of 2.5% and country's at 2.7% at the time. But the effect of the outreach program became even more pronounced over the winter, as the tribe and health workers gained access to monoclonal antibody treatments, according to Close. He said the high-risk outreach team started referring patients for antibody treatment in December as part of their protocol after the therapy received emergency use approval from the Food and Drug Administration. Hospital staff at the Whiteriver hospital then administered the antibody treatment. "We give that to people who are asymptomatic or mildly ill to prevent hospitalization," Close said. "The evidence currently suggests that reduces the risk that they're going to get sicker and get hospitalized and reduces the risk that they're going to die." Though there's no data proving the antibody treatments made a difference, Close said that after health care workers started using them, the community's COVID-19 death rate fell to 0.5%. Hospital workers also gave antiviral therapies, such as remdesivir, to patients early and often. "We probably overtreated some people," he said. "But the good news is it definitely led to significant reductions in mortality." Lessons for the future Close believes the different programs were so successful because health care workers were often able to test, trace, diagnose and treat individuals all in the same day — a feat he said was only possible because of how closely integrated hospital workers and community health workers were. "There were no barriers in communication between the public health arm of our response and the clinical care arm of our response," Close said. "It's really a case for an integrated health care system." As the tribe emerges from the pandemic and tribal members get vaccinated against the virus, Close said the hospital may start exploring other health conditions where it can use the high-risk outreach team, which is already trained and experienced in clinical evaluations. "The goal is to take what we've learned from COVID and now apply it to things that are not COVID-related," Close said. Another valuable lesson Close hopes to carry forward is how much of a difference visiting residents in their homes can make and how important building trusting relationships with the community is. Nashio said going door to door to trace and monitor COVID-19 cases was a natural step for CHRs, who had already gone door to door in the past for other community health campaigns. "We know firsthand how difficult it can be to not only connect with patients over the phone but communicate effectively over the phone," Nashio said. "When the community sees their CHRs coming to their door, it helps decrease the stigma of the disease." In addition to performing checkup evaluations and providing information, Nashio said CHRs can also provide food, medical supplies, cleaning supplies or services like grocery shopping and running basic errands. Not every tribal member has reliable internet or phone service, nor access to transportation, so Close said going door to door can be a good way to reach, and help, everyone. "Meeting patients where they are is invaluable," Close said. Amanda Morris covers all things bioscience, which includes health care, technology, new research and the environment. Send her tips, story ideas, or dog memes at amorris@gannett.com and follow her on Twitter @amandamomorris for the latest bioscience updates. Independent coverage of bioscience in Arizona is supported by a grant from the Flinn Foundation. -
 2021-03-04
2021-03-04What pandemic? One urbanite's weekend venture into rural Arizona
In addition to all the other aspects that currently define my life, I can almost see the end of my first year of graduate studies in Arizona State University's Global History program. I returned to academia in the fall of 2019, wrapped up 34 undergrad credit in 9 months with a 4.1 GPA, and started my master's studies in the fall of 2020. I still have to work a dayjob to keep the lights on, and I have a side hustle ghost writing fiction novels and hosting a podcast on creative writing. Time is my most valued and least possessed commodity. My school schedule is generally comprised of 7.5-week courses, and the university recommends taking no more than one at a time. I couldn't avoid doubling up during the first two months of this spring semester, and, to be candid, I arrogantly denied the validity of the university's guidance. By the end of the first term, I desperately needed to remember what a weekend felt like. Because God blessed me with the Greatest Wife in The History of the World, she scheduled a four-day weekend for us in the White Mountains in eastern Arizona. For those unfamiliar with the area, eastern Arizona has the largest stand of Ponderosa pine trees in the world. Hunters consistently harvest trophy elk and deer from the White Mountains and Gila National Forest, which spans the Arizona-New Mexico border. Unlike Colorado's coniferous forest, eastern Arizona seems devoid of pine beetle kill. Nothing but healthy, evergreen forest and the scent of sun-warmed pine greets you. We stayed in a vacation home on the outskirts of Pinetop, brought our groceries from home, and largely intended on hiking, cooking, drinking, and doing a lot of nothing. When we arrived in Pinetop in early March 2021, I had already fully recovered from COVID-19 and had time for both of my Moderna vaccines to have taken full effect. My wife had neither protective barrier, but we had generally become comfortable with purpose-driven shopping (as opposed to "window shopping") and takeout dining. As such, we stopped into a bakery to get breakfast on the way out to the hiking trails as a vacation treat. To our surprise, many of the patrons weren't wearing masks while walking through the restaurant or waiting in line. That made us a little uncomfortable. Then, one of the employees walked out from the kitchen with no mask on and began working on filling orders at the front, cold-food storage counters. Both of us panicked a bit and considered cancelling our orders and leaving. My wife pulled up the Arizona Department of Health Services site and quickly found that entire county had endured only a little more than 560 cases. A quick bit of division translated that into an average of two infections per day for the entire pandemic year-to-date. The statistical odds of the unmasked clerk or patrons presenting a health risk to either of us fell to just north of zero. NOT zero, but we both felt we could see it from there. The ham, egg, and cheese croissants were delicious, by the way. In trying to be good guests, we continued to wear our masks whenever we ventured into public spaces and businesses. Less than half of those around did the same, and I didn't see or hear anyone confront each other about mask wearing. Our last venture out that weekend was to a beer garden with a prominent outdoor patio and seating area. We again wore our masks inside the establishment, but we immediately felt like outcasts for having done so. When we stepped inside, it looked as though the town villain had just stepped through the saloon doors: all activity inside the business stopped, and everyone seated inside turned around to look us up-and-down for few silent moments. If anyone had been playing piano, they would have switched to a minor key. NO ONE else inside wore a mask, and the interior tables didn't appear to have been spaced to comply with prevailing social distancing guidelines. Everyone stayed kind of quiet until we ordered beers and asked to sit outside. In hindsight, I wonder if they expected we were there from some government bureaucracy to issue citations, or just out-of-towners about to have a value-based hissy fit? I have been generally opposed to broad behavior mandates that typically justify compliance on urban problems, but that weekend compelled me to really consider the divergent pandemic realities Arizonans have endured for the past year. Further analysis of county-specific data seems to suggest at least four divergent pandemic experiences within Arizona: urban centers, border counties, rural counties, and Native American reservations. I hope to better understand the personal experiences of those who lived in these diverse regions and how the pandemic affected their perspective and reality. -
 2021-03-25
2021-03-25News Article: Graham County (AZ) now with less than 150 active documented COVID-19 cases
"By Jon Johnson, jonjohnsonnews@gmail.com SAFFORD – Graham County has had very few new confirmed cases of COVID-19 in the past month, lowering its numbers to just 147 active cases as of Thursday. According to the Graham County Department of Health and Human Services, Graham County has had a total of 5,355 confirmed cases for the course of the pandemic, with 5,132 listed as being recovered, 147 active, and 76 deaths in more than a year. No new cases were recorded Thursday, and, according to the Arizona Department of Health Services COVID-19 school dashboard, Graham County had just a 1 percent positivity rate as of the week of March 14. That is good for a tie with Apache County for the second-lowest percent positivity rate out of Arizona’s 15 counties. Only Greenlee County, which registered a zero percent positivity rate from Feb. 27 – March 14, had lower. With the lower cases statewide and vaccine rollout, Governor Doug Ducey issued an Executive Order on Thursday, rolling back several COVID-19 mitigation measures involving businesses and gatherings. This comes as other states roll back their COVID-19 mitigation measures as well. The rollout of the various COVID-19 vaccines has picked up steam in the last month, with the state opening up the vaccine to anyone 16 years old or older for the Pfizer vaccine. Anyone 18 years old or older can be administered the Moderna and Johnson & Johnson vaccines. The San Carlos Apache Healthcare Corporation is holding a free, drive-through vaccine clinic on Saturday, March 27 at the San Carlos High School. No appointment is necessary. The clinic will be administering both the Pfizer and Moderna vaccines. Graham County and Greenlee County are also providing vaccination sites for those 18 and older, and provide the Moderna and Johnson & Johnson vaccines. Greenlee County: According to the Greenlee County Health Department, the county currently has just nine active cases of COVID-19. For the course of the pandemic, Greenlee County has had 568 confirmed positive cases (by far the lowest out of any of Arizona’s 15 counties), with 549 recovered cases, nine active, and 10 deaths." -
 2021-03-30
2021-03-30News Article: Greenlee County (AZ) down to just 2 active COVID-19 cases
"By Jon Johnson, jonjohnsonnews@gmail.com GREENLEE COUNTY – The Greenlee County Health Department reported Monday that the county had just two confirmed active cases of COVID-19. Greenlee County has tested more than 5,000 people for the course of the pandemic and has had a total of 568 cases, with 556 recovered and 10 deaths. The county offers the Moderna COVID-19 vaccine to all residents 18-years-old or older, and on Thursday (01-April-2021) Gila Health Resources will have a vaccine clinic for the one-shot Johnson and Johnson COVID-19 vaccine. Click here to learn more or to register. According to the Arizona Department of Health Services, 37.5 percent of Greenlee County’s residents have been vaccinated for COVID-19. That is the highest percentage out of Arizona’s 15 counties. Conversely, Graham County is listed as having just 18.1 percent of its population vaccinated, which is the third-worst out of Arizona’s counties behind Maricopa County at 17.5 percent and Apache County at 10.7 percent. Graham County: The Graham County Department of Health and Human Services reported three new confirmed positive tests for COVID-19 on Tuesday. While Graham County has had 5,364 total confirmed cases of COVID-19, as of Tuesday the county had just 138 confirmed active cases. Out of all its confirmed cases, 5,150 are listed as being recovered, and 76 have died. Graham County is also offering both the Moderna and Johnson & Johnson vaccines to all residents 18-years-old or older. Click here for more information." -
 2021-04-05
2021-04-05Greenlee County (AZ) Health Department's Daily COVID-19 Updates through April 5, 2021
The Greenlee County Health Department uses its Facebook page to disseminate daily information related to the COVID-19 pandemic to its residents. The daily COVID-19 statistics are displayed as an image on the daily Facebook post, which allows examination of the department's content and messaging before and after the pandemic. Governor Doug Ducey declared a state of emergency in Arizona on March 11, 2020, which seems inconsistent with GCHD's daily posts from that period. Language on the GCHD posts consistently advised residents to stay home if they felt ill, rather than being consistent with Governor Ducey's voluntary Stay Home orders. For example, the March 30, 2021, press release to update a new active COVID-19 infection in Greenlee County reads as follows: "For Immediate Release, Tuesday, March 30, 2021, Greenlee County, Arizona. Public Information Contact: Steve Rutherford (928) 865-2601 NEW RELEASE - COVID-19 Positive Test in Greenlee County The Greenlee County Health Department is investigating one (1) new confirmed case of COVID-19. The case will put our current total at five hundred and sixty-nine (569) confirmed Greenlee County COVID-19 cases... We would like to remind the community to use masks appropriately when outside of the home, practice social distancing, wash your hands frequently, and do not go into the public when you are feeling sick, unless you are seeking medical attention." These updates demonstrate a significant dichotomy between the rural and urban experiences during this pandemic. -
 2021-03-30
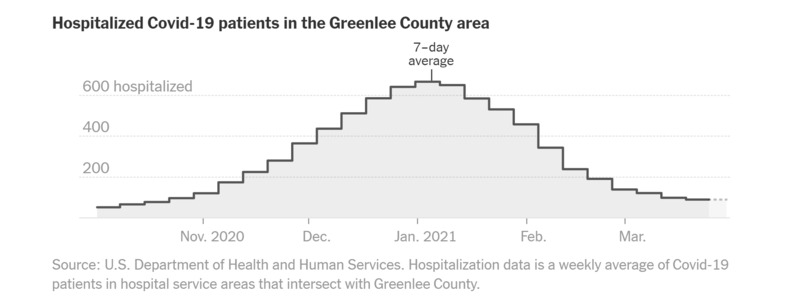
2021-03-30A Tale of Two Arizonas: COVID-19 Data from Maricopa and Greenlee Counties Through March 30, 2021
This daily tracker displayed on the New York Times site displays and explains public data provided by the Arizona Department of Health Services. The attached graphs illustrate the disparate COVID-19 experience between Arizona residents in Maricopa County and Greenlee County. Arizona is the sixth largest of the United States with a population of more than seven million residents within its 113,594.08 square miles. 61% of Arizonans reside in Maricopa County, which translates to a population density of approximately 481.3 people per square mile, or 57,959.3 square feet per resident. In contrast, southeastern Arizona’s Greenlee County claims only 0.14% of the state’s residents for a population density of 5.7, or approximately 4.8M square feet per person.