Items
topic_interest is exactly
variant
-
 2021-07-13
2021-07-13New daily COVID-19 cases in US have doubled in past 3 weeks
The COVID-19 curve in the U.S. is rising again after months of decline, with the number of new cases per day doubling over the past three weeks, driven by the fast-spreading delta variant, lagging vaccination rates and Fourth of July gatherings. Confirmed infections climbed to an average of about 23,600 a day on Monday, up from 11,300 on June 23, according to Johns Hopkins University data. And all but two states — Maine and South Dakota — reported that case numbers have gone up over the past two weeks. -
 2021-04-16
2021-04-16India's escalating COVID numbers
India has seen an explosion in their reported infection numbers recently. This Medscape article explained that India has recently crossed the 200,000 daily infections mark which puts India as the highest infection rate in the world. The article then explained how at India's largest Covid facility, Lok Nayak Jai Prakash Narayan Hospital, they are past full capacity. It is so bad that they are putting two unrelated patients in the same bed to maximize their patient capacity. This is truly unimaginable! The hospital's medical director, Suresh Kumar, expressed that it is the new variants and human behavior that has caused the recent spike in numbers. Hopefully this is not a preview for what is in store for the rest of the world. -
 2021-04-07
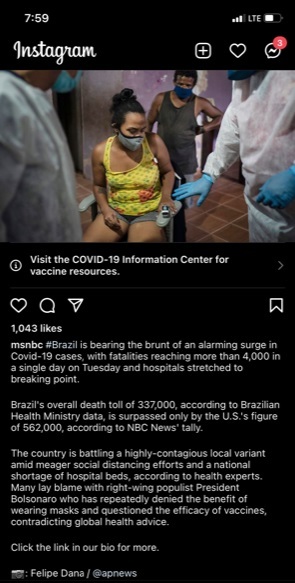
2021-04-07Brazil is Bearing the Brunt of an Alarming Surge
MSNBC reports on an alarming surge in Brazil and how it is trying to deal with a local variant and its politicians who still deny the severity of COVID-19. -
 2021-04-08
2021-04-08Covid update from India
A friend shares an update on how Covid is currently affecting India and the new measures put in place to control the spread. He adds information on the US consulate because he is a US citizen living in India. -
 2021-04-06
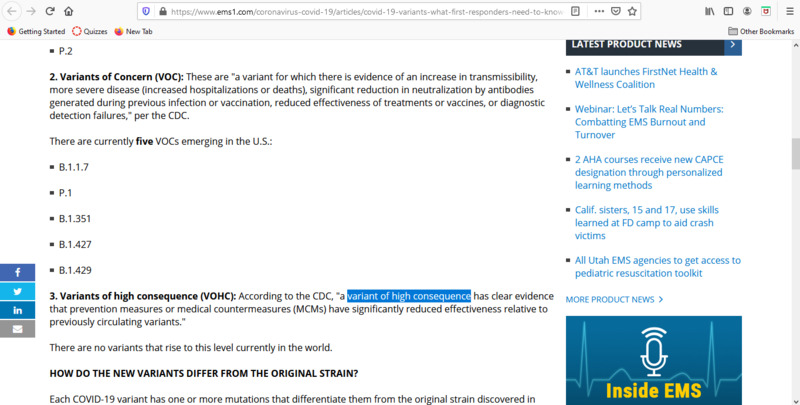
2021-04-06COVID-19 variants
This is an article about the variants of COVID-19 that are either present or emerging in the United States. It is meant to keep EMS providers informed with up-to-date information so that they can provide the best care to patients. Some of the variants are more dangerous/have more symptoms than others. It notes that there is 5 variants of concern, which have increased transmissibility and increased hospitalizations/deaths. While this is not great news, it is a good thing that there are currently no variants in the world that are considered variants of high consequence by the CDC, which essentially means that medicine does not have effective means of treating it. Hopefully this remains the case and we can start to see a drop off of the variants of concern soon. -
 2021-04-17
2021-04-17North Dakota begins testing sewage for COVID-19 variants
Like many other states, North Dakota has started to test their sewage for COVID-19 variants. Although the testing can't track down the virus to specific households, it can determine if the city still has COVID-19 and what variants are present. -
 2021-04-01
2021-04-01News Article: ASU watching new COVID-19 'Arizona variant' with a mutation known to weaken vaccines
By Amanda Morris of the Arizona Republic: Arizona State University researchers have found a home-grown variant of the coronavirus emerging in Arizona that they say should be monitored closely because it carries a mutation known for weakening vaccines. In a non-peer reviewed study that published Sunday, researchers said they have detected 17 cases of the new variant since February, 15 of which were in Arizona. The other two cases were found in Houston in late February and New Mexico in early March, suggesting that the variant has begun to spread. "My hope is that we do not see more of these cases. The whole point of surveillance is to keep this from spreading," said Dr. Efrem Lim, an ASU virologist and assistant professor. The variant is known as the B.1.243.1 variant, and descends from a common lineage of the virus called B.1.243, which nationally makes up about 2.5% of all cases, according to David Engelthaler, director of the Translational Genomics Research Institute's infectious disease division in Flagstaff. "It's not dominant. But, there's a fair amount of that lineage that has been able to hang around," Engelthaler said. "It seems to have picked up this E484K mutation, what we call the 'eek!'" This E484K mutation has also been seen in the variants first detected in South Africa and Brazil, as well as one new variant recently discovered in New York. Numerous studies have shown that this mutation — located in the spike of the virus — lowers antibody responses to the virus and could weaken vaccines. Antibodies are one of the body's tool to recognize and fight the virus. The E484K mutation has been shown to weaken antibody responses. One study from Seattle showed that it caused the neutralizing effects of antibodies to decrease by tenfold, and numerous other studies have shown similar results. American vaccine development company Novavax reported that its COVID-19 vaccine was 96.4% effective against the original coronavirus strain and 86.3% effective against the U.K. variant, but was far less effective in South Africa, where the South Africa variant carrying this mutation is dominant. In the South Africa trials, the vaccine was shown to be 48.6% effective overall, and 55.4% effective in HIV-negative individuals. Moderna announced a sixfold reduction in antibody responses from its vaccine against the South Africa variant, and Pfizer observed a drop in vaccine-induced antibody responses against the South Africa variant. The Johnson & Johnson vaccine is reported to be 64% effective against moderate to severe COVID-19 in trials in South Africa vs. 72% effective in U.S. trials. Though the E484K mutation appears to reduce antibody response and possibly reduce vaccine efficacy, Lim stressed that vaccines still work well and said people should get their vaccines as planned. Scientists are monitoring mutations in the spike of the novel coronavirus. Community spread is a concern Though the new Arizona variant carries this mutation, it's still possible for the variant to fizzle out and stop spreading. Lim said researchers have found two other cases where viruses within the B.1.243 lineage independently picked up the E484K mutation, but did not spread. "In both cases, they never led to more transmissions," Lim said. Engelthaler has also tracked other lineages where the E484K mutation showed up, but those strains fizzled out. Overall, researchers have detected over 60 samples containing the E484K mutation statewide, according to TGen's Arizona COVID-19 sequencing dashboard. In order to continue spread, Engelthaler said variants need to be very "fit." "This mutation has popped up on multiple instances and then just goes away," he said. "This one mutation by itself doesn't give the virus superpowers." "It’s definitely a mutation of concern but time will tell if it will be a variant of concern," he added. If the mutation shows up in a more fit version of the virus, then Engelthaler said it becomes more of a concern. The new variant in Arizona is different than past cases because it has already spread from one person to another and could spread further, according to Lim. He said "one-off" mutations here and there are normal, but that the bigger question is about the transmission levels of this variant. A variant's ability to spread to others is also dependent on human behavior, Lim said. If people follow public health guidelines, they are less likely to spread variants to others. In total, Lim said the new Arizona variant has 11 mutations, which is "quite a bit more" than normal virus variations. These 11 mutations could be helping the virus survive or spread and could also act as a "fingerprint" to help researchers identify the new variant, Lim said. Another one of the 11 mutations is located in the spike that the virus uses to attach to and infect cells. Engelthaler said that because of the importance of the spike, any mutations in that area could affect things like how fast the virus spreads or how severe the related illness is. Both Lim and Engelthaler said it's too soon to tell whether the other mutations in this variant have any effect. Overall, this variant still seems to account for a very low percentage of overall cases in the state, according to Dr. Joshua LaBaer, the executive director of ASU's Biodesign Institute. ASU researchers wrote that it's still possible there are more undetected cases of the variant since there are limited efforts to genetically monitor the virus nationwide. In Arizona, roughly 1.3% of cases overall have been genetically sequenced, or analyzed, according to TGen's Arizona COVID-19 sequencing dashboard. In February and March, over 3% of cases were sequenced, higher than national rates of sequencing, which were below 1% in January. ASU is working with the Arizona Department of Health Services to monitor the new variant and hopefully prevent further spread through contact tracing and other public health measures, Lim said. California and UK variant cases rise Currently the Arizona variant is only considered a "variant of interest" and not a "variant of concern." These are different categories outlined by the CDC and used to assess the risk level of each variant. The CDC defines "variants of interest" as those that are associated with potential changes, whereas "variants of concern" have evidence showing actual changes such as increased transmission, more severe disease or antibody evasion. There are five variants of concern, which include variants first identified in the United Kingdom, South Africa, Brazil and California. Two variants from California were elevated from variant of interest to variant of concern this month and have rapidly spread in Arizona. "They're closely related to each other and have definitely been documented with increased transmissibility and some impact on some antibody treatment," Engelthaler said. In November 2020, both the California variants accounted for only 0.73% of Arizona's genetically sequenced samples. By March, they accounted for 31.64% of samples and are predominant variants statewide. One non-peer reviewed study from the University of California San Francisco showed weaker antibody responses against the California variants. Because of concerns that monoclonal antibody treatments may be less effective against these two variants, the U.S. Department of Health and Human Services announced two weeks ago that it would limit the distribution of one treatment to states with high levels of the California variant, including Arizona. The California Department of Public Health also recommended that the state stop distributing the treatment, which is made by American pharmaceutical company Eli & Lily. In a health alert, the department said this treatment was unlikely to be active against the California variants. The U.K. variant, which is highly contagious, has also been spreading statewide ever since it was first detected in late January. In March the U.K. variant accounted for 4.72% of genetically analyzed samples. Currently, Engelthaler said Arizona has over 100 cases of the U.K. variant and over 1,000 cases of the California variants. Arizona also detected its first cases of the South Africa variant last week. So far, Lim said that all of the variants of concern are manageable and have not risen to the level of "variant of high consequence," which the CDC defines as variants that are shown to significantly reduce the effectiveness of prevention and medical measures. "The risk is whether one of these current variants of concern acquire additional mutations that push it up to the next level," Lim said. To prevent further mutations, LaBaer said it's important to prevent spread of the virus by continuing to follow health guidelines and getting vaccinated. The more the community can prevent the spread of the virus, the less mutations will occur, he said. "We're kind of in this race right now between the developed dominance of these much more infectious variants that are now spreading throughout the country and getting people vaccinated," LaBaer said. "At the moment, I'm a little worried that the spread of this virus is so fast that that may outpace our ability to get vaccines in arms." He said it was theoretically possible that new variants could escape the vaccines, meaning that the public would move backward away from reaching herd immunity. But Lim said the vaccines can easily be updated to protect against new variants. Pharmaceutical companies like Pfizer and Moderna are already working on developing updated booster shots. In the meantime, researchers will continue to monitor the Arizona variant to see if it spreads further. Engelthaler said he expects the most fit variants of the virus to become more dominant statewide as people continue to get vaccinated and stamp out less successful strains. "There's a bit of a race here with the virus — a survival of the fittest race," Engelthaler said. "But what we don't want is to raise too much concern that things are going in the wrong direction...what we're doing is closely watching the evolution of a virus like we never have before. It's good that we have this capability, it's more important to put it into context." Amanda Morris covers all things bioscience, which includes health care, technology, new research and the environment. Send her tips, story ideas, or dog memes at amorris@gannett.com and follow her on Twitter @amandamomorris for the latest bioscience updates. Independent coverage of bioscience in Arizona is supported by a grant from the Flinn Foundation. -
 2021-04-04
2021-04-04News Article: How a local response to COVID-19 helped slow deaths on the White Mountain Apache nation
By Amanda Morris of the Arizona Republic: When someone on the Fort Apache Indian Reservation receives a confirmed diagnosis of COVID-19, health care workers from the Whiteriver Indian Hospital jump into action. They personally visit the individual's home to test other household members, perform health evaluations on everyone there and trace any other potential contacts at risk for COVID-19 exposure. Health care workers in the community say that could be one reason why, even though the rate of confirmed COVID-19 cases among White Mountain Apache tribal members is nearly triple the state's rate, the death rate is much lower and continues to fall. Over 90% of COVID-19 cases in the White Mountain community are investigated within 24 hours of testing, according to Ryan Close, the director of the Department of Preventative Medicine at the Whiteriver hospital, which is the only hospital on the 1.67 million-acre reservation. "I feel like what we did made a huge difference," Close said. "We evaluated and admitted people aggressively and early. The tribe deserves an incredible amount of credit for mobilizing staff ... to make this response possible, because at some point it would have been very difficult to maintain without their considerable help." The quick response may have also helped the tribe turn the tide against rapid community spread of the virus, which scientists say could have been fueled by a single variant found only in the White Mountain tribal communities. The variant carried a mutation in the spike protein, which scientist theorize could have made it spread more rapidly than other strains of the virus. The number of confirmed COVID-19 cases among White Mountain Apache tribal members accounts for 24% to 28% of their population, according to Close, but the cumulative death rate among known cases is only 1.2%. By comparison, the statewide rate of infection was 11.5% with a 2% death rate among known cases. And over the winter, Close said the rate for the tribe dropped even lower, to about 0.5%. In a community with a high number of individuals with underlying health conditions, the low death rate and work of the tribe has been "remarkable," said David Engelthaler, director of the Translational Genomics Research Institute's infectious disease division in Flagstaff. The death rate also stands out as unusually low when compared with death rates in other Indigenous communities. Indigenous populations have been disproportionally affected by the pandemic. CDC data shows that Indigenous people are 3.5 more likely to be diagnosed with COVID-19 and almost twice as likely to die from COVID-19 than white people. Close credits a proactive strategy to combat COVID-19 that involved rapid contact tracing, in-person health evaluations and frequent outreach to high-risk COVID-19-positive individuals as well as early treatment with monoclonal antibodies and other antiviral therapies. Volunteers and health workers from the White Mountain Apache community were on the Whiteriver hospital's contact tracing team and high-risk COVID-19 outreach team, which Close said helped the team connect better with the people and work faster. One essential part of the team are the tribe's community health representatives, or CHRs, who are members of the community that serve as a cultural bridge between patients and medical establishments. JT Nashio, director of the Community Health Representatives for the tribe, said the "visceral connection" that CHRs have to the community helps them bring cultural awareness to the way questions are asked for contact tracing, which makes the process more effective and allows officials to better distribute information. "On top of that, quite simply, they know how to get around. It’s a big reservation and not all homes are easy to find," Nashio said. "But when you’ve lived here your whole life, you know where to find people. That became invaluable during the tracing and testing push during case surges." Virus mutation may have made it more transmissible When COVID-19 hit the White Mountain Apache nation, it spread rapidly. The community's first documented case was on April 1, 2020, from someone who had likely recently visited the Phoenix area, unknowingly caught COVID-19 and returned, according to Engelthaler. Within the first few weeks, Close said the community experienced a handful of deaths. "We soon had incidence rates that were skyrocketing. Case counts were going up very, very quickly," Close said. It's unclear why the disease spread so rapidly in the community, but the initial strain of COVID-19 that hit the community carried a mutation that Engelthaler believes could have made it more transmissible. "They were seeing the virus just rip through and have an 80 to 90 to 100 percent attack rate," he said. TGen partnered with the tribe and the U.S. Indian Health Services early on to provide tests to diagnose a case of COVID-19 and provide genetic analysis of the virus from each case. It showed one strain of the virus circulating in the tribal community that wasn't present anywhere else in the state. "This virus moved much faster than anything else we were seeing in Arizona at the time," Engelthaler said. "So we actually believe that we had one of these variant strains in Arizona that was causing very large numbers of cases, but it was secluded and maintained really only in that tribal population." The mutation, called the H245Y mutation, occurred in the spike of the virus, which Englethaler said is a "very sensitive" part of the virus where mutations can have a significant impact. Because of the low death rate, Engelthaler said TGen researchers would like to investigate the mutated strain of coronavirus seen among tribal members to see if it is also associated with a lower fatality rate. He acknowledged that other strains of the virus have since entered the community and that the actions of health care workers in the community and at the Whiteriver hospital is also responsible for the lower death rates. 'The earlier you treat an illness, the better' Close's biggest concern was that an outbreak would cause a "tsunami" of sick COVID-19 patients that would run the risk of overwhelming the Whiteriver hospital, which does not have an intensive care unit. Any patients that require intensive care need to be transported to other hospitals in the state. "We're a small hospital, we cannot take a wave of all very acute patients because there aren't enough ventilators in the hospital," Close said. "There aren't enough helicopters in the state to transport people out from our facility to a higher level of care." Within the first few weeks, Close said the community experienced a handful of deaths, and patients who had the poorest outcomes were the ones who self-presented at the hospital — often meaning they waited until they felt sick enough to go to the hospital. "People don't always bring themselves in early enough," Close said. "The earlier you treat an illness, the better." In response to this phenomenon, the hospital started a high-risk outreach program the third week of April. Health care workers regularly visited the homes of anyone who tested positive for COVID-19 and was at high risk for a poor outcome. Close recalls multiple days when he evaluated patients and found their oxygen levels dangerously low, even though they felt fine. It's a condition associated with COVID-19 known as "silent hypoxia," or "happy hypoxia." "They had no sense that they were even ill. They went on to get pretty sick in the hospital, but they survived and you can't help but think to yourself, 'Yeah, that's a life saved,'" Close said. "That person, if they had stayed home another day or another two days would not have done as well. They would have ended up on a ventilator or something." The Arizona Republic previously reported that the effects of the high-risk outreach program and contact tracing led to a fatality rate among tribal members of 1.6% last June, which was less than the state's rate of 2.5% and country's at 2.7% at the time. But the effect of the outreach program became even more pronounced over the winter, as the tribe and health workers gained access to monoclonal antibody treatments, according to Close. He said the high-risk outreach team started referring patients for antibody treatment in December as part of their protocol after the therapy received emergency use approval from the Food and Drug Administration. Hospital staff at the Whiteriver hospital then administered the antibody treatment. "We give that to people who are asymptomatic or mildly ill to prevent hospitalization," Close said. "The evidence currently suggests that reduces the risk that they're going to get sicker and get hospitalized and reduces the risk that they're going to die." Though there's no data proving the antibody treatments made a difference, Close said that after health care workers started using them, the community's COVID-19 death rate fell to 0.5%. Hospital workers also gave antiviral therapies, such as remdesivir, to patients early and often. "We probably overtreated some people," he said. "But the good news is it definitely led to significant reductions in mortality." Lessons for the future Close believes the different programs were so successful because health care workers were often able to test, trace, diagnose and treat individuals all in the same day — a feat he said was only possible because of how closely integrated hospital workers and community health workers were. "There were no barriers in communication between the public health arm of our response and the clinical care arm of our response," Close said. "It's really a case for an integrated health care system." As the tribe emerges from the pandemic and tribal members get vaccinated against the virus, Close said the hospital may start exploring other health conditions where it can use the high-risk outreach team, which is already trained and experienced in clinical evaluations. "The goal is to take what we've learned from COVID and now apply it to things that are not COVID-related," Close said. Another valuable lesson Close hopes to carry forward is how much of a difference visiting residents in their homes can make and how important building trusting relationships with the community is. Nashio said going door to door to trace and monitor COVID-19 cases was a natural step for CHRs, who had already gone door to door in the past for other community health campaigns. "We know firsthand how difficult it can be to not only connect with patients over the phone but communicate effectively over the phone," Nashio said. "When the community sees their CHRs coming to their door, it helps decrease the stigma of the disease." In addition to performing checkup evaluations and providing information, Nashio said CHRs can also provide food, medical supplies, cleaning supplies or services like grocery shopping and running basic errands. Not every tribal member has reliable internet or phone service, nor access to transportation, so Close said going door to door can be a good way to reach, and help, everyone. "Meeting patients where they are is invaluable," Close said. Amanda Morris covers all things bioscience, which includes health care, technology, new research and the environment. Send her tips, story ideas, or dog memes at amorris@gannett.com and follow her on Twitter @amandamomorris for the latest bioscience updates. Independent coverage of bioscience in Arizona is supported by a grant from the Flinn Foundation. -
 2021-01-14
2021-01-141 person dies every 6 minutes: How L.A. became the nation's largest coronavirus hot spot
LOS ANGELES — In Los Angeles County, 10 people on average test positive for the coronavirus every minute. Every six minutes, someone dies from Covid-19, according to county public health data. The startling figures come as Los Angeles became the first county in the nation to record 1 million confirmed coronavirus cases since the start of the pandemic. According to county public health officials, roughly 1,003,923 people in L.A. have been infected with the virus and more than 13,000 people have died. The numbers are equally sobering across the state. California has nearly 2.9 million confirmed coronavirus cases and more than 31,000 deaths, according to NBC News counts. A more contagious variant of the virus has also been detected in the region. -
 2021-03-09
2021-03-09Navajo Nation outpacing states in rate of vaccinations
By Rima Krisst | Mar 9, 2021 | CORONAVIRUS, News | WINDOW ROCK President Jonathan Nez proudly said last week that the Navajo Nation had exceeded its goal of administering 100,000 COVID-19 vaccine shots by end of February, crediting tireless health care workers who have been serving seven days a week to plan vaccinations and administer the vaccines. On Tuesday, the president’s office reported that 135,161 COVID-19 vaccine shots have gone into arms on the Navajo Nation, which represents 92% of the total 146,980 doses received and includes 48,800 persons who have had their second shots. This means that over 26% of the approximately 327,000 enrolled Navajos have gotten a shot through the Navajo Area Indian Health Service and tribal health care system, which is an amazing feat. By comparison, in New Mexico 22.4% of the population (738,705) has been given at least one shot. Arizona has administered at least one shot to 17.1% of the population (1,847,750), with Utah trailing behind at 12.2% receiving at least one shot (687,925), according to the CDC data vaccine tracker. And as of March 2, 15.3% of the U.S. population had received at least one shot, with 76.9 million shots administered, including 25.4 million receiving the second dose. Approximately 1.8 million vaccines per day are being administered daily in the U.S. So, percentage-wise, Navajo is outpacing both neighboring states and the general U.S. population. ‘Amazing partnership’ On a Feb. 25 IHS media call, IHS Chief Medical Officer Rear Adm. Michael Toedt reported that as of Feb. 18 the IHS had also achieved its goal of administering 400,000 doses of COVID-19 vaccine “across IHS, tribal, and urban Indian Health programs,” representing 16% of the “target population,” with 6.3% receiving two doses. “This milestone was reached ahead of schedule despite severe weather, making travel to health facilities difficult across much of Indian Country and leading to shipping delays,” said Toedt. Toedt said most IHS facilities have now vaccinated the majority of their priority populations and are moving into Phase 2, which includes those who work in higher risk settings such as schools and prisons. “Very shortly we expect that everyone who needs a vaccine will be able to receive it,” he said. Toedt credited IHS and tribal health care employees across the country who are committed to ensuring the protection of tribal communities in 11 geographic areas covering 26 states and 349 health facilities, many in rural and remote locations. “We have had an amazing partnership with our tribes to use all available resources to help with delivery of vaccine,” said Toedt. This included distribution and redistribution of vaccines by ground and air transportation as needed. Toedt said the IHS has also conducted over 2 million COVID-19 tests at a higher per capita than most states and is reporting a seven-day average test positivity rate of 4.5%, below the 5.6% all-races rate in the U.S., despite the fact that COVID-19 has had a disproportionate impact on American Indians/Alaska Natives. The Navajo Nation has conducted 245,085 COVID-19 tests resulting in 29,774 positive cases. ‘Developing trust’ Coordinated public relations campaigns in partnership with tribes have been key to the success of the vaccine rollout, said Toedt. Navajo Area IHS Chief Medical Officer Loretta Christensen agreed, saying public messaging has been critical. “This collaboration is one of the reasons we’ve been extremely successful,” said Christensen. “Honesty and transparency, developing that trust with the people you are serving is vital. We have spent a great deal of time on that relationship with our Navajo people to encourage them to be vaccinated.” She said the communication process has been very unified across Navajo and with the president’s office, using social media, radio, and a bilingual approach. “This is constant public education,” she said. “We encourage people in a very personal way that we would like them to be safe, keep their families, their communities safe. We feel very fortunate and grateful that our population has really stepped up.” Toedt acknowledged there has been some vaccine hesitancy relating to how quickly the vaccines were developed and whether or not they are completely safe, which has made some people distrustful. According to IHS Public Affairs Specialist Joshua Barnett, a recent IHS-funded survey by the Urban Indian Health Institute reported that 75% of Native Americans were willing to get a vaccine and 74% believe that doing so is their responsibility to help protect their community. “I’m confident that the process for vaccine development has the full integrity and completeness of time necessary to make sure these vaccines are safe, but it’s our job as healthcare providers to communicate that in a way that’s acceptable and trusted by our population,’ said Toedt. “We know our efforts are working and we’re seeing good delivery and acceptance of these vaccines in our communities.” Reaching the homebound Christensen said one of the strongest assets in the Navajo vaccination campaign has been the collaboration between public health nurses and community health representatives in reaching out to community members at the local level, including homebound elders and persons with disabilities. “These are the people out in the rural areas that know the families, that know the homes,” said Christensen. “We rely on them for that person-to-person contact out in the communities.” She said between 4,000 to 5,000 homebound individuals have actually been vaccinated at home or close to home. Moving forward with the goal of getting the Navajo population vaccinated and achieving “community immunity,” Navajo Area IHS wants to make sure that all 27,000 square miles of the Nation have been penetrated, said Christensen. “We want to be able to target any communities, populations or subgroups that have perhaps maybe not been able to get vaccinations,” she said. “So, our first step is to heat-map our whole area and then focus on those populations that are perhaps more rural or don’t have easy access to healthcare facilities.” “Our goal is to get every single person vaccinated and to keep our populations in Arizona, New Mexico and Utah safe,” she said. Christensen said her team will be working with chapters to identify anyone who might have been missed. They have also reached out to Navajos living off reservation and have established an online registry to help people find a place to get their vaccination. “We highly encourage them to come back if they need to and we will certainly take care of them and their families,” she said. Tracking variants In regard to surveillance for COVID-19 variants, Toedt said IHS does contribute its tests to state public health labs as well as different large lab corporations such as TriCore, LabCorp. and additional processes for genomic testing are in development. “The samples that are included through those mechanisms are sampled through the CDC’s processes to test for genomics,” said Toedt. Christensen said similarly the Navajo Area and the Health Command Center are working to establish more specific genomic surveillance within Navajo Nation. “In the meantime, we are participating in testing both in New Mexico and Arizona,” said Christensen. Christensen said the Navajo Epidemiology Center has also reached out to bordering states requesting any relevant information on variants be shared. “We all stand by ready to support this process and we are hopeful that we will have more specific information for Navajo Nation very soon,” she said. Christensen confirmed that she was not aware of any variants having been identified on the Navajo Nation from random sampling. “We have requested that information but we have not received it as of yet,” she said. Adverse events Any adverse events, or serious side effects, related to vaccinations within IHS are collected and reported to the same CDC system that collects the data nationally, said Toedt, but the data broken down by individual tribes is not publicly available. “We are part of that Vaccine Adverse Event Reporting System through the CDC,” said Toedt. “All adverse drug reactions are investigated by the CDC to determine what category it goes in and how they analyze data.” Navajo Area is gathering information on any adverse events on the Navajo Nation, but there are patient privacy issues when it comes to sharing that publicly, said Christensen. “We do, as (health care) institutions across Navajo Nation, share basic data with each other when we’re doing best practices,” she said. Christensen would not answer whether or not there had been any adverse events on the Nation. “I will say we have done very well with these vaccines,” she said. “There are certainly side effects which have been well defined, but we’ve had minimal significant adverse events. I cannot quantify that for you, but we are tracking those events across Navajo Nation.” Preventing transmission As far as keeping everyone safe after being vaccinated, Toedt said it’s still important to continue to wash your hands, stay six feet apart and to wear a mask. This is because vaccinated persons can theoretically still contract COVID-19 and spread it after being vaccinated, although they may not have any symptoms due to protection from the vaccine. There are also still many unknowns related to COVID-19 variants and to what extent they may evade vaccine protection, be more transmissible, or cause more serious disease. “We have been trying to report on possible variants most recently, explaining that we don’t have all the information yet on what the long term effects of those variants are,” said Christensen. “So we highly suggest that you still watch your distance, wash your hands and wear your mask.” Christensen said public messaging encouraging everyone to abide by the public health protocols in place, regardless of vaccination status, will continue until there is community immunity. -
 2021-03-16
2021-03-16Why America should help vaccinate the world against COVID-19: 'This is not charity'
With new COVID-19 variants appearing, the WHO and GAVI have teamed up to give vaccines to countries that are having difficulties obtaining them. The United States has given $4 billion to cause. -
 2021-02-13
2021-02-13Canada is 'playing chicken' with COVID-19 by reopening while variants are spreading widely
Many are criticizing provinces plan's to continue to open up as Covid-19 variants are springing up throughout the country. Places like Quebec have begun to reopen businesses such as museums, malls, and hair salons while having a curfew in place. Newfoundland is facing a current surge with a variant strain.